(Swedish not yet below)
There seems to be a consensus that placebo* is something that ”happens” while (a) the knowledge of this process is largely (almost) non-existent and (b) the main use of science is to try to eliminate it (sugar pillplacebo). Since drugs must try to show that it is precisely the drug that has an effect, they try in different ways (unfortunately, some studies have been discovered to cheat) show through different methodological designs that drugs ”beat” the placebo effect, which is not always the case. Thus, elimination and increased knowledge dominates multidisciplinary science / knowledge-wise and its clinical individual-based use! Unfortunately, this creates an ”elimination negative attitude” (Limbic automatically imprinted through education contract cluster).
At the same time, we can thus assume that the placebo effect (unusually high degree of ignorance in relation to the general knowledge on which medicine / psychology / psychiatry rests – again, absolute knowledge base – still) works but has not been shown interest, perhaps not only because some found way to make money on some ”Placebo-Strategy-Treatment”.
NOTE, also that we often don’t even mention nocebo, which is placebo’s opposite supposed effects.
Below I discuss from a completely reverse perspective where placebo and nocebo constitute the most important thing to try to increase knowledge about and to also gradually do innovative clinical studies (which absolutely cannot harm and give side effects not only as symptoms but excite or worsen physiological dysfunctions.
Assumptions
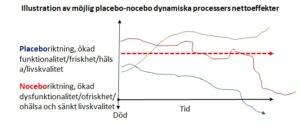
1. Placebo and nocebo can be (a) only psychological dynamic process that does not affect physiological systems dynamic (or static, however now it can happen, but something that often drugs do) and (b) psychophysiological dynamic processes where thus (postulated via Limbic spatial processes) also physiological processes are affected, in placebo positive and nocebo negatively BUT where also a form of antagonism (antagonism is an interaction between organisms where one organism benefits at the expense of another. This includes predation, or a predator eating prey. Think of bears killing salmon. It also includes parasitism, or one organism depending on (but not killing) a host https://study.com/academy/lesson/antagonism-definition-biology.html ) prevails
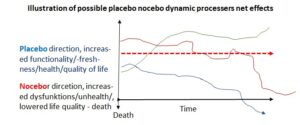
We can assume
that placebo/nocebo not only varies within and between individuals but also across situations and time – i.e., dynamic processes
– That these dynamic processes are largely (or completely?) not directly conscious and/but Limbic constantly updating reconsolidating external and internal inputs in relevant constract clusters that in turn affect or do not affect (to varying degrees) biological systems
– That people in principle also have different (as above) propensity to react with dynamic placebo/nocebo behaviors, which makes it extremely complex but at the same time perhaps crucial for developing a system integrated multidisciplinary biopsychosocial medicine understanding, because it follows the principle that complex systems processes should be influenced as high up in the hierarchies as possible. Thus, it also means that we can expect that effectively influencing placebo/nocebo processes also consist of strategies that operate (Limbic conditioning reconsolidating) high up in biopsychosocial strategic behavior hierarchies
that…
Even more complex is what is present (of ”placebo and nocebo factors/behaviors”) and what is absent (of them). So, a seemingly placebo effect can be a down regulation of one (or more) existing nocebo(s) and vice versa!
More text coming
* Common definition: …
My own opinion is expressed at (although needed to be updated) Placebo R&D | Biopsychosocial Medicine